Extremely high triglycerides in FCS can lead to a high risk of acute pancreatitis1,2
European guidelines suggest that fasting triglycerides (TGs) ≤10 mmol/L (880 mg/dL) reduces the risk of acute pancreatitis (AP)1To prevent recurrence, the International Association of Pancreatology (IAP) guidance recommends maintaining triglyceride levels below 5.7 mmol/L (500 mg/dL)3
People with Familial Chylomicronaemia Syndrome (FCS) can experience a range of complications, such as:4
- Nausea
- Vomiting
- Eruptive xanthomas
- Lipaemia retinalis
- Hepatosplenomegaly
- Recurrent acute pancreatitis
- Recurrent episodes of abdominal pain
Among these, severe and recurring episodes of acute pancreatitis represent the greatest burden4–6
Recurring episodes of acute pancreatitis are also highly burdensome for healthcare systems. Multiple episodes of acute pancreatitis can damage the pancreas, leading to chronic pancreatitis and diabetes2,7,8
The PRIMARY GOAL of FCS treatment is to reduce acute pancreatitis risk1,7,9
Affecting more than 50% of people with FCS, acute pancreatitis is the most severe potentially fatal complication.8 To reduce the risk of acute pancreatitis, the primary goal of FCS treatment is lowering triglyceride levels to a clinically significant threshold1,7
Retrospective cohort study reporting the annualised incidence rate of acute pancreatitis from a nationally representative US ambulatory electronic medical records database (N=7,119,195)2
*The data represents the overall cohort (all patients), including individuals with no acute pancreatitis events, one event, or ≥2 events in the past 12 months. Data are not specific to people with FCS2
Identifying those at risk of acute pancreatitis caused by high triglycerides is critical, because even one acute pancreatitis event dramatically increases the chance of a future one2
Maintaining triglycerides below 5.7 mmol/L (500 mg/dL), as recommended by the IAP, reduces the risk of recurrence3
Just one meal can increase acute pancreatitis risk
Accumulation of chylomicrons (chylomicronaemia) from dietary fat can increase acute pancreatitis risk after just one meal10,11
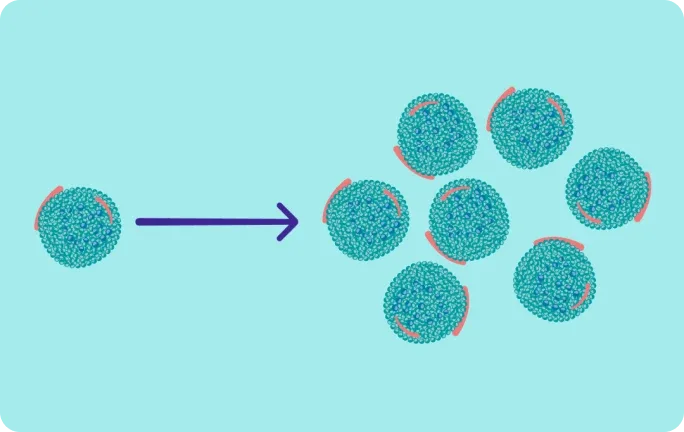
Triglycerides clearance can be saturated, and the body may be unable to clear additional dietary chylomicrons11
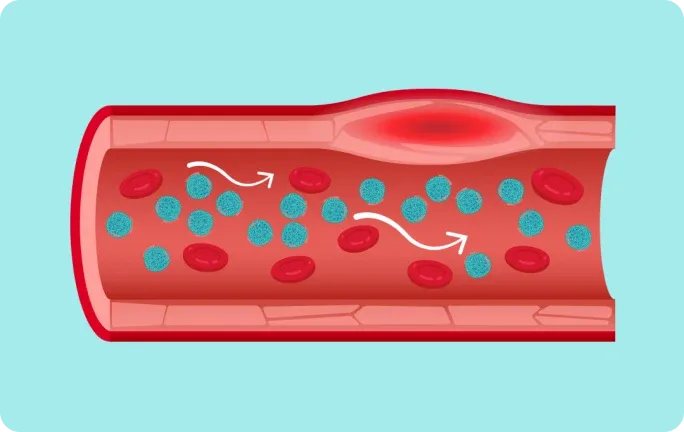
High levels of chylomicrons (chylomicronaemia) are thought to restrict blood flow and induce inflammation11,12
The pancreas may be particularly vulnerable to ischaemic damage caused by high levels of chylomicrons11,12

Among people with extremely high triglycerides, as seen in FCS, what proportion have experienced an acute pancreatitis event?*4,13
Thank you for your response.
*Data from hypertriglyceridaemia cohort studies13
Physical and emotional toll of acute pancreatitis
People with FCS report significant psychosocial burdens associated with recurrent acute pancreatitis.4,9 One of the most common emotional symptoms of FCS is constant uncertainty about the possibility of acute pancreatitis or pain4
People with FCS report that their disease impacts their mental well-being and social lives4
In a survey of 166 people with FCS, one of the most common emotional symptoms is constant uncertainty about the possibility of acute pancreatitis or pain4
Uncertainty about acute pancreatitis or pain
34%
Anxiety, fear, or worry about health
26%
Uncertainty about what or how to eat
20%
Feeling out of control because of their FCS
17%
GUIDELINES & EXPERT OPINION POINT TO THE NEED TO AIM LOWER1,3,14,15
Reduce Acute Pancreatitis risk
Aim for ≤10 mmol (880 mg/dL)1
ESC/EAS Guidelines and NLA expert opinion suggest that lowering triglyceride levels to ≤10 mmol (880 mg/dL) reduces the risk of acute pancreatitis1,14
FURTHER REDUCE RISK & PREVENT RECURRENCE
Aim below 5.7 mmol/L (500 mg/dL)3
International guidelines recommend maintaining triglycerides below 5.7 mmol/L (500 mg/dL) in people with extremely high triglycerides:
- The Endocrine Society/European Society of Endocrinology Clinical Practice Guidelines: to help further reduce risk of acute pancreatitis15
- IAP: to help prevent recurrence of acute pancreatitis3
How can you aim lower to reduce acute pancreatitis risk in people with FCS?
Sign up for updates and more information
Receive further disease state information on FCS and its impact
Abbreviations
AP, acute pancreatitis; EAS, European Atherosclerosis Society; ESC, European Society of Cardiology; FCS, Familial Chylomicronaemia Syndrome; IAP, International Association of Pancreatology; NLA, National Lipid Association; TG, triglyceride.
Show References
- Mach F, Baigent C, et al. Eur Heart J. 2020;41(1):111–88.
- Sanchez RJ, Ge W, et al. Lipids Health Dis. 2021;20(1):72.
- Párniczky A, Mikó A, et al. Pancreatology. 2025;25(6):770–814.
- Davidson M, Stevenson M, et al. J Clin Lipidol. 2018;12(4):898–907.
- Gelrud A, Williams KR, et al. Expert Rev Cardiovasc Ther. 2017;15(11):879–87.
- Larouche MB, Watts GF, et al. Curr Opin Endocrinol Diabetes Obes. 2025;32(2):75–88.
- Shamsudeen I, Hegele RA, et al. Expert Rev Clin Pharmacol. 2022;15(4):395–405.
- Guda NM, Tikudanathan G, et al. Lancet Gastroenterol Hepatol. 2018;3(10):720–8.
- Gaudet D, Stevenson M, et al. Lipids Health Dis. 2020;19(1):120.
- Paragh G, Németh Á, et al. Lipids Health Dis. 2022;21:21.
- Goldberg RB, Chait A, et al. Front Endocrinol (Lausanne). 2020;11:593931.
- de Pretis N, Amodio A, et al. United European Gastroenterol J. 2018;6(10):649–55.
- Hernandez P, Passi N, et al. Curr Atheroscler Rep. 2021;23(11):65.
- Javed F, Hegele RA, et al. J Clin Lipidol. 2025;19(3):382–403.
- Newman CB, Blaha MJ, et al. J Clin Endocrinol Metab. 2020;105(12):3613–82.