Take aim at an important cause of extremely high triglycerides1–5
Familial Chylomicronaemia Syndrome (FCS) causes extremely high triglycerides (TGs) that are not lowered adequately by conventional triglyceride-lowering approaches (e.g., fibrates, statins, and omega-3 fatty acids)6–9
FCS CAUSES EXTREMELY HIGH TRIGLYCERIDES6–9
Extremely high triglycerides can be caused by genetic, metabolic, and lifestyle factors.8,10 Consistent fasting triglyceride levels above 10 mmol/L (880 mg/dL) could be a sign of an underlying disease, such as FCS5,6
If extremely high triglycerides persist despite conventional approaches and lifestyle changes, consider FCS as the cause5,6
Not an actual patient
What is FCS?
FCS is a rare disorder with a global prevalence of 1 to 13 per 1,000,000. It may have a genetic cause, characterised by the absence of functional lipoprotein lipase in 80% of cases, but it is not always explained by known genetic causes11
Most conventional triglyceride-lowering approaches activate lipoprotein lipase, which is missing or non-functional in people with an underlying disorder such as FCS7–9,12
In unaffected individuals, lipoprotein lipase clears circulating triglycerides and chylomicrons from the blood shortly after a meal.4 In people with FCS, loss of lipoprotein lipase activity leads to the accumulation of triglycerides and chylomicrons (chylomicronaemia), resulting in fasting triglyceride levels at 10x-100x the normal level (fasting triglycerides above 10 mmol/L [880 mg/dL] to over 22.6 mmol/L [2000 mg/dL]) that may only marginally lower with conventional triglyceride-lowering approaches2–4
Suspect FCS in people with extremely high triglycerides
Many cases of FCS are misdiagnosed because the nature of extremely high triglycerides is misunderstood. People with FCS tend to present with symptoms that are shared with other conditions – often experiencing acute pancreatitis attacks with no clear triggers9,13,14
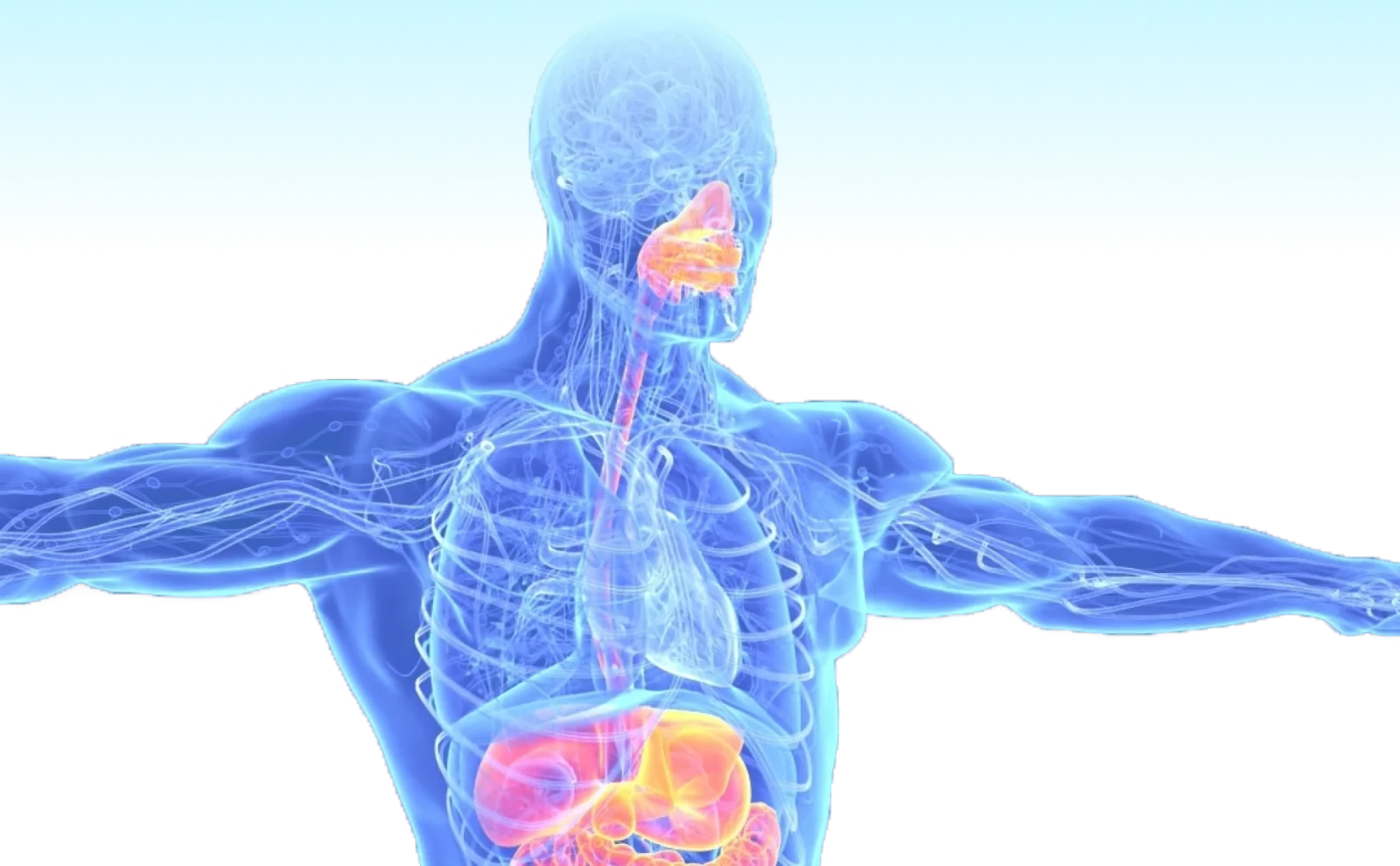
In addition to causing acute pancreatitis, FCS can impact the liver, spleen, heart, eyes, and cause other systemic problems9
Symptoms and comorbidities reported in a survey of 166 people with FCS:9
Tap the green hotspots to learn more
- Difficulty concentrating (16%)
- Impaired judgment (11%)
- Lipemia retinalis (9%)
- Brain fog (8%)
- Forgetfulness (8%)
- Abdominal pain (41%)
- Acute pancreatitis (40%)
- Bloating (37%)
- Indigestion (27%)
- Diabetes (16%)
- Chronic pancreatitis (11%)
- Hepatomegaly (Enlarged liver, 11%)
- Splenomegaly (Enlarged spleen, 10%)
- Hypertension (10%)
- Feeling of physical weakness (asthenia, 30%)
- Eating disorders (23%)
- Fatigue (23%)
- Peripheral neuropathy (7%)
FCS CAN BE DIAGNOSED BOTH CLINICALLY AND GENETICALLY15,16
People with extremely high triglycerides that do not respond to conventional triglyceride-lowering approaches may display clinical characteristics similar to FCS, but have no clear genetic cause5,15,16
However, clinical manifestation of FCS, including treatment resistance and acute pancreatitis, can also have a multifactorial, polygenic cause5,15
Clinical confirmation of FCS
Factors that can clinically characterise FCS and may warrant referral to specialists include:13,15,16
Persistent triglyceride levels above 10 mmol/L (880 mg/dL)
Prior history of acute pancreatitis
Recurrent hospitalisations for severe abdominal pain without other explainable cause
History of childhood pancreatitis
Family history of hypertriglyceridaemia-induced acute pancreatitis
In cases of recurrent acute pancreatitis, consider a diagnosis of FCS4,16–18
Aim for early diagnosis and referral
The sooner people with suspected FCS are referred to specialists (e.g., lipids specialists, endocrinologists, and cardiologists holding lipid expertise), the sooner the underlying cause of elevated triglycerides can be diagnosed. Holistic support from a dedicated healthcare team can aim to lower the risk of acute pancreatitis by lowering triglyceride levels to ≤10 mmol/L (880 mg/dL)1,14,17,18
Common misconceptions could delay diagnosis
Identify FCS at the first signs with this guide to FCS fact‑checking
Not an actual patient
Do you want to find out more about complications related to FCS?
Lower Acute Pancreatitis Risk1,14,16,19,20
Sign up to learn more about acute pancreatitis risk in FCS
Abbreviations
AP, acute pancreatitis; FCS, Familial Chylomicronaemia Syndrome; mRNA, messenger ribonucleic acid; TG, triglyceride.
Show References
- Mach F, Baigent C, et al. Eur Heart J. 2020;41(1):111–88.
- Larsson M, Vörsjlö E, et al. J Biol Chem. 2013;288(47):33997–4008.
- Blom DJ, O'Dea L, et al. J Clin Lipidol. 2018;12(5):1234–43.
- Gaudet D, Brisson D, et al. N Engl J Med. 2014;371(23):2200–6.
- Goldberg RB, Chait A, et al. Front Endocrinol (Lausanne). 2020;11:593931.
- Paragh G, Németh Á, et al. Lipids Health Dis. 2022;21:21.
- Spagnuolo CM, Hegele RA, et al. Expert Rev Endocrinol Metab. 2024;19(4):299–306.
- Gouni-Berthold I. J Endocr Soc. 2020;4(2):bvz037.
- Davidson M, Stevenson M, et al. J Clin Lipidol. 2018;12(4):898–907.
- Virani SS, Morris PB, et al. J Am Coll Cardiol. 2021;78(9):960–93.
- Pallazola VA, Sajja A, et al. Eur J Prev Cardiol. 2020;27(19):2276–80.
- Veliadkis N, Stachteas P, et al. Pharmaceuticals (Basel). 2024;17(5):568.
- Javed F, Hegele RA, et al. J Clin Lipidol. 2025;19(3):382–403.
- Falko JM. EndocrPract. 2018;24(8):756–63.
- Larouche MB, Watts GFC, et al. Curr Opin Endocrinol Diabetes Obes. 2025;32.
- Moulin P, Dufour R, et al. Atherosclerosis. 2018;275:265–72.
- Stroes E, Moulin P, et al. Atheroscler Suppl. 2017;23:1–7.
- Witztum JL, Tsimikas S, et al. J Clin Lipidol. 2023;17(3):342–55.
- Santos RD, Watts GF, et al. J Clin Lipidol. 2021;15(4):620–4.
- Brown WV, Goldberg IJ, et al. J Clin Lipidol. 2018;12(2):254–63.