
Not an actual patient.
Learn more about the experience of FCS
Familial Chylomicronaemia Syndrome (FCS) affects everyone differently. Symptoms can vary over time and may disrupt your daily life, even when you otherwise feel well1
Physical experiences
People with FCS commonly have triglyceride levels that are 10 to 100 times higher than normal (17–170 mmol/L [1,500–15,000 mg/dL]).2 When your body has too many triglycerides in the blood, it can affect you in different ways.3

Not an actual patient
Generalised abdominal pain is one of the most common experiences for people with FCS. This may range from mild discomfort to more noticeable pain and is often felt in the upper abdomen. While it can be unsettling, this type of pain is a recognised part of living with very high triglyceride levels. Other symptoms and health problems commonly associated with FCS can include:3
- Acute pancreatitis
Acute pancreatitis
Acute pancreatitis is an inflammation of the pancreas that typically causes sudden, severe upper abdominal pain, sometimes radiating to the back.1,3
- Abdominal pain
- Enlarged liver and/or spleen
- Physical weakness
- Fatigue
- Nerve pain or numbness in your hands and feet
- Diabetes
- Bloating
- Indigestion
- Eating disorders
- Problems thinking
Problems thinking
Difficulty concentrating, impaired judgment, brain fog, and forgetfulness.3
- Eye problems
Eye problems
Lipaemia retinalis: Blood vessels in the retina appear thin and creamy white or salmon-coloured.1–3
- Fatty lumps on your body
Fatty lumps on your body
Eruptive xanthomas: Firm, raised, and waxy-appearing bumps on the torso or extremities.1,3
Acute Pancreatitis is a complication of fcs
Acute pancreatitis is a sudden inflammation of the pancreas and is one of the most serious complications associated with FCS.1 However, the risk can be reduced by managing very high triglyceride levels.1,4
Not everyone with FCS will experience acute pancreatitis, and the risk can vary from person to person.1 However, acute pancreatitis is a serious condition that requires urgent medical attention, so it's important to seek help straight away if you develop sudden, severe abdominal pain.1,2
Chylomicrons and the risk of pancreatitis
Your body creates particles called chylomicrons from fat in your diet. Chylomicrons move triglycerides to where your body needs them.5
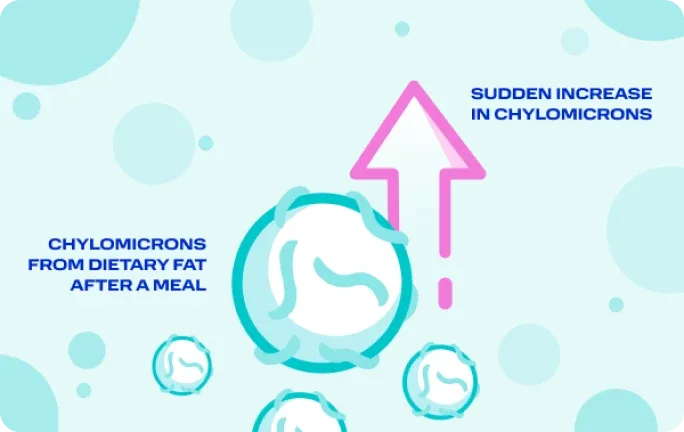
A buildup of chylomicrons from dietary fat can overwhelm the body.6
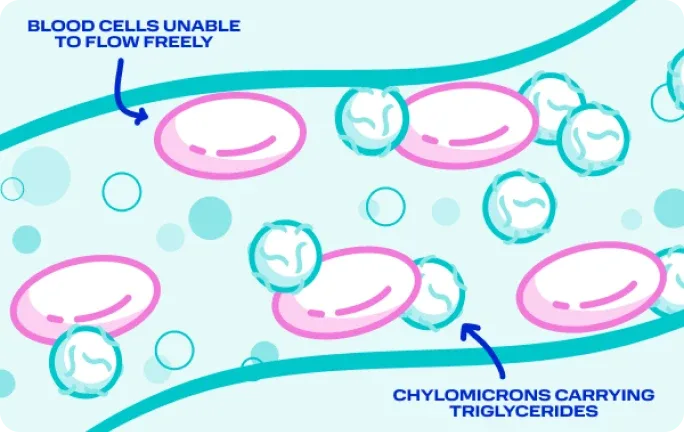
The sudden rise in chylomicron levels may reduce blood flow and trigger inflammation.6–8
High levels of chylomicrons in the blood may cause pancreatic inflammation and flares.8–9
Illustrations created for educational purposes based on information described in Qui et al 2023. This is a simplified example of the mechanism of action.
What are the risks of acute pancreatitis?
Having one episode of acute pancreatitis may increase the likelihood of further episodes for some people. Over time, repeated episodes can affect how the pancreas works and may lead to longer-term pancreatic problems.10,11
*Overall number of cases (n) ranged from 185 in the >11.3 mmol/L group to 4,111 in the <2.3 mmol/L group.11
Reducing triglycerides may help reduce risk of pancreatitis flares12
Very high triglycerides can cause acute pancreatitis, which is a sudden inflammation of the pancreas leading to painful attacks.13 Although acute pancreatitis can be severe, the risk can often be reduced with the right management and by working towards appropriate triglyceride goals with a healthcare professional.4
Scientific research shows that lower triglyceride levels are linked with a lower risk of acute pancreatitis. A big impact on reducing risk is seen with triglyceride levels at or below 10 mmol/L (880 mg/dL), with lower triglyceride levels linked to an even lower risk.4,11
Triglyceride levels could be related to pancreatitis flares. Do you know your average fasting triglyceride level?
Please select your response. Your answer is confidential
Thank you for your response.
People with triglycerides above 10 mmol/L (880 mg/dL) are at risk of acute pancreatitis.4 Speak to your doctor about what you can do to decrease your levels.
See your risk
Not an actual patient.
GOAL
Triglycerides levels below 10 mmol/L (880 mg/dL)12
A guideline task force of experts from the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS) – representing fields such as cardiology, endocrinology, and lipidology – agree that keeping triglyceride levels below 10 mmol/L (880 mg/dL) reduces the risk of acute pancreatitis.4
By partnering with your doctor to work towards the guideline triglyceride level, you could reduce your risk of acute pancreatitis.4
Emotional Impact
Living with a rare condition like FCS can be challenging. Symptoms may be unpredictable, and getting a diagnosis can take time. This can sometimes lead to feelings of fear, anxiety, and helplessness.3 Understanding how FCS can affect everyday life may help people feel more confident sharing their experiences with family, friends, and healthcare professionals.
Diet is one of the most important factors in FCS14
If you are living with FCS, sticking to a very low-fat diet is central to managing the condition14
Know what to expect
Knowing the possible signs and symptoms help you have more informed conversations with your healthcare team
Want to hear from people who are living with FCS?
Abbreviations
CI, confidence interval; FCS, Familial Chylomicronaemia Syndrome.
Show References
- Action FCS. Symptoms of FCS. Available at: https://www.actionfcs.org/about-fcs/symptoms-of-fcs/. Last accessed May 2026.
- Gaudet D, Brisson D, et al. N Engl J Med. 2014;371(23):2200–6.
- Davidson M, Stevenson M, et al. J Clin Lipidol. 2018;12(4):898–907.e2.
- Mach F, Baigent C, et al. Eur Heart J. 2020;41(1):111–88.
- Feingold KR, Grunfeld C, et al. Endotext. South Dartmouth (MA): MDText.com, Inc.; 2000.
- Goldberg RB, Chait A, et al. Front Endocrinol (Lausanne). 2020;11:593931.
- Chait A, Brunzell JD, et al. Endocrinol Metab Clin North Am. 2022;51(3):539–55.
- de Pretis N, Amodio A, et al. United Eur Gastroenterol J. 2018;6(10):649–55.
- Qiu M, Zhou X, et al. Clin Nutr. 2023;42(5):3692–700.
- Falko JM, O’Connor CM, et al. Endocr Pract. 2018;24(8):756–763.
- Sanchez RJ, Escobar C, et al. Lipids Health Dis. 2021;20(1):72.
- Grundy SM, Stone NJ, et al. J Am Coll Cardiol. 2019;73(24):e285–e350.
- Gapp J, Tariq A, et al. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024.
- Stroes E, Moulin P, et al. Atheroscler Suppl. 2017;23:1–7.